Anterior Cruciate Ligament (ACL) Injury Intermediate Exercise Programme
Aim to perform this programme a minimum of once per day unless prescribed otherwise. As with any new exercise, start slowly (repetitions as able) and build up as you are able within the guidelines below.
Pain should not exceed 4/10 whilst completing this exercise programme.
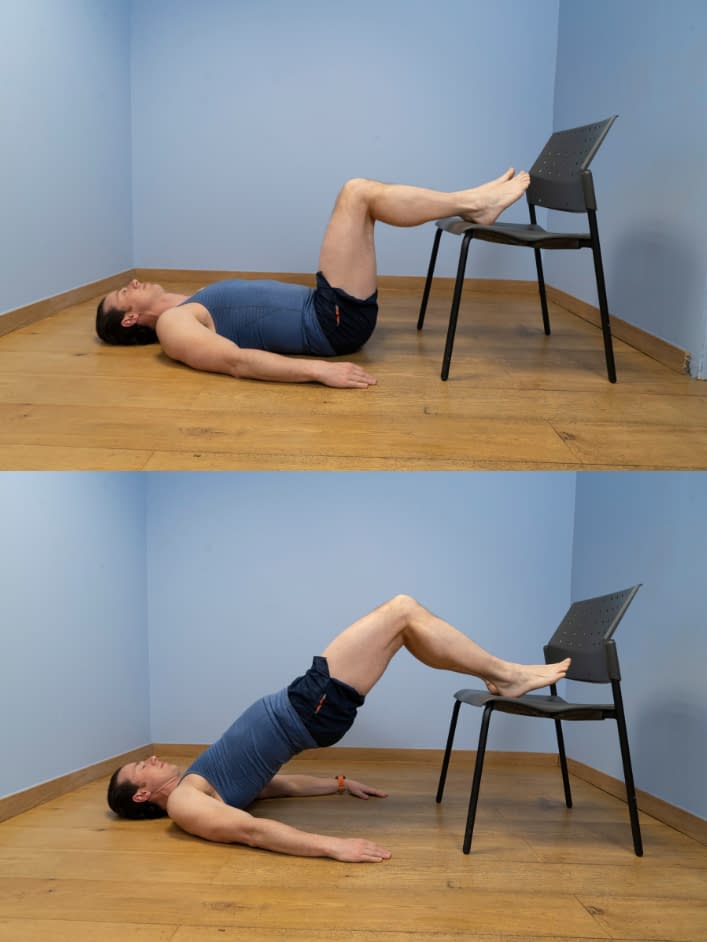
1. Hip bridge with feet elevated
- On a comfortable surface, lay flat on your back with your knees bent and heels placed on a raised platform such as a box or a chair – have the feet and knees hip-width apart.
- Raise your hips up towards the ceiling by pushing digging in your heels and squeezing your buttock muscles.
- Once your hips form a straight line with the shoulders and knees, hold for 5 seconds before slowly lowering your hips back down.

2. Supported squat
- Start with the feet shoulder width apart and hold onto a stable object (e.g., Bannister or kitchen sink) at about waist height.
- From this position bend your knees and sit backwards as if you are sitting into a chair.
- As you do so lean slightly forwards at the hips so that your head stays over your feet.
- Make sure that your weight is going through your heels at all times.
- Go as low as you feel comfortable but no lower than your thighs parallel with the floor.

3. Single leg balance
- Perform this exercise barefoot or in socks, in a clear space near a wall/stable object and on a flat, non-slip surface.
- Shift your weight on to the affected leg then lift the supporting leg slightly off the floor – maintain a slight bend in the standing knee.
- Look down at the knee and focus on balancing whilst keeping the knee in line with the hip and ankle – use the object/wall to prevent yourself falling.
- Aim to hold your balance for up to 1 minute or until reaches 4/10 on your pain scale.
- To progress, try looking straight ahead rather than down at the knee. To advance further, this can be performed with the eyes closed.
We recommend consulting a musculoskeletal physiotherapist to ensure exercises are best suited to your recovery. If you are carrying out an exercise regime without consulting a healthcare professional, you do so at your own risk. If you have any concerns whilst completing these exercises, please contact a healthcare professional.
More Plans
The primary goals post-operatively are the reduction of swelling and pain, and to normalise your walking pattern and patella mobility as soon as possible. The physiotherapist will prescribe exercises to regain knee extension and flexion within the first few days post-operatively. Full knee extension should be retained as early as possible, ideally within the first few weeks, and knee flexion should be regained fully within the first 6 weeks.
Quadricep activation exercises should start within the first few days post-operatively, progressing onto closed kinetic chain exercises at the knee between 0-60º. It is important that we do not solely focus on the knee joint and look to strengthen the entire lower limb including the glute, calf and hamstring with exercises focusing on muscle hypertrophy.
Cardiovascular training on a static bike can begin when 100º of knee flexion is achieved and neuromuscular training should begin in the first few weeks (8,9). Pain should not exceed 3/10 on your perceived pain scale whilst completing this exercise programme.
- 0
- 1
- 2
- 3
- 4
- 5
- 6
- 7
- 8
- 910
In the later stages of rehabilitation, you will start to develop your single-leg multi plantar and multisegmental movements. This is important to develop as the role of your injured anterior cruciate ligament is to prevent multi-planar movements. Sports-specific rehabilitation should begin involving visual-motor training (15). Strength and power work must continue through the intermediate and advanced stages of rehabilitation, making sure there is the incorporation of exercises addressing the limb’s rate of force development. It is important to be strong and powerful but, as peak anterior cruciate ligament strain can be seen very early on in a movement (within less than a second), it is important that our muscles are not only strong but are able to react quickly to protect the ligaments from excessive pressures (14). Pain should not exceed 4/10 whilst completing this exercise programme.
- 0
- 1
- 2
- 3
- 4
- 5
- 6
- 7
- 8
- 910